Cindy L. Hunter (cindy.hunter@tmf.org) is a Healthcare Quality Improvement Specialist III, Karen S. Sabharwal (karen.sabharwal@tmf.org) is an Analytic Consultant IV, and Jay Crosson (jay.crosson@tmf.org) is a Quality Improvement Executive at TMF Health Quality Institute in Austin, TX.
In 2018, the Centers for Medicare & Medicaid Services (CMS) projected that improper payment for post-acute care (PAC) services provided through the Medicare Fee-for-Service program totaled $8.3 billion, with home health services accounting for more than 30% of these payments.[1] Submitting insufficient documentation or failing to adequately document medical necessity are the main reasons for these improper payments. To help address this problem, CMS provides free provider-level reports comparing service use and billing to state-level, jurisdiction-level, and national aggregate data through the Program for Evaluating Payment Patterns Electronic Report (PEPPER). PEPPERs summarize Medicare claims data across areas prone to improper payment. CMS distributes these reports to short-term acute care providers once every quarter and to other types of hospitals and PAC providers once every year. Providers can use PEPPERs to inform their compliance programs; for example, providers can use this information to prioritize areas for auditing and to review their billing practices for Medicare services. These reports also support PAC providers in their participation in Medicare’s new Prospective Payment Systems (PPSs) for PAC.
CMS made modifications to the inpatient rehabilitation facilities’ (IRFs) PPS and launched a new PPS for skilled nursing facilities (SNFs) in October 2019. CMS also launched a new PPS for home health agencies (HHAs) in January 2020. These changes pay PAC providers based on patient mix and resource use as part of CMS’s efforts to reduce reliance on volume-based payment models. The new PPS for SNFs, the Patient Driven Payment Model, focuses on patient characteristics rather than volume of therapy to classify patients and improve payment accuracy. CMS also modified the PPS for IRFs, including units in short-term acute care hospitals and critical access hospitals, to reflect refinements in case mix adjustments. As of January 2020, HHAs participate in the PPS for the Patient Driven Groupings Model. This model includes case mix adjustments to account for comorbidities, changed the existing 60-day episode payment to a 30-day period payment, and takes account of the admission source when calculating prospective payments.
PEPPER updated
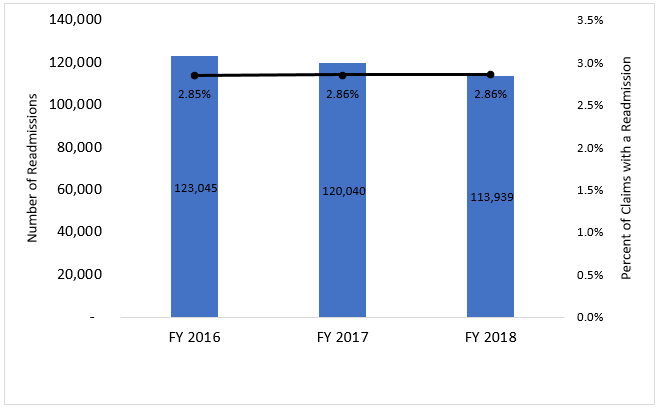
To address the PPS-related changes, CMS is updating PEPPER as well. The updated PEPPER is a free report comparing PAC provider billing to other PAC providers of the same type—in addition to comparisons of national, state, and jurisdictional-level trends—using three years of Medicare Fee-For-Service billing data. The RELI Group, along with its partners, TMF Health Quality Institute and CGS, produces PEPPERs on behalf of CMS. For SNFs, PEPPERs now include data on readmissions. In particular, these data focus on the percentage of readmissions within three to five calendar days (or four to six consecutive days) to the same facility for the same beneficiary for episodes ending during the reporting period. These data assess compliance with the new interrupted stay policy introduced in October 2019. Figure 1 displays data collected over the past three fiscal years for three- to five-day readmissions in SNFs.
Home health agencies
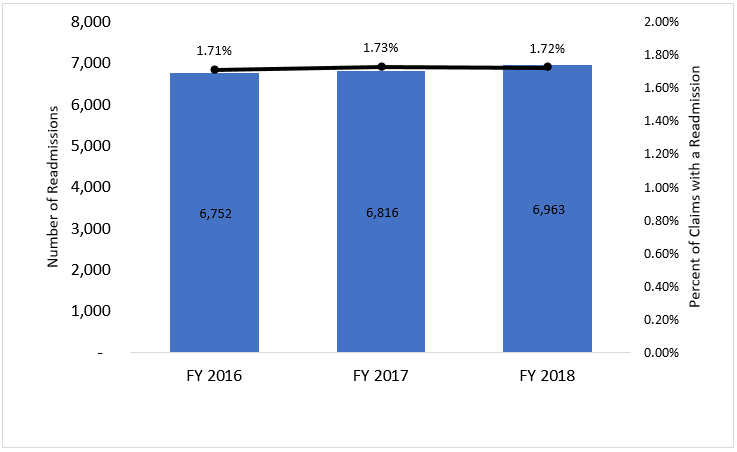
For HHAs, PEPPERs will soon include performance data on three new measures. Approximately 85% of HHAs will have access to PEPPERs that include comparative data regarding payments for patients with a condition that qualifies for a low comorbidity adjustment. In addition, HHAs will have access to PEPPERs with data on HHA periods qualifying for high comorbidity adjustment payments, along with comparative billing data for periods with an institutional referral source. For IRFs, PEPPERs now include two new measures. First, the reports include comparative data regarding the percent of discharged patients with a length of stay in the facility that is less than or equal to three days. Second, the IRF PEPPERs include the percentage of readmissions to the same IRF that occur within three to five calendar days (or four to six consecutive days) for the same beneficiary. Figure 2 displays data collected over the past three fiscal years for three- to five-day readmissions in IRFs.
While this year’s PEPPER releases for SNFs and IRFs reflect these changes, the new HHA PEPPERs will require data from 2020 and will not change until 2021. As the new PEPPERs become available, PACs should take the opportunity to review their billing patterns for these new target areas and the use patterns of the Medicare Fee-For-Service beneficiaries they serve. By doing so, PACs should be able to identify areas where they may be at risk of improper billing. If a PAC provider identifies potentially improper billing practices, the PEPPER support team can assist with answering any of the provider’s questions. Using its PEPPER, the provider may conduct an internal audit of its coding, billing, and documentation to evaluate resource use and ensure the delivery of medically necessary care. PACs may then use this information to develop a quality improvement plan focused on improving the efficiency, effectiveness, and outcomes of care. For more information on PEPPER, visit pepper.cbrpepper.org. Please submit any questions or requests for assistance through the PEPPER Help Desk on the website homepage.
Takeaways
-
Centers for Medicare & Medicaid Services (CMS) changed the payment classification system for skilled nursing facilities and inpatient rehabilitation facilities in October 2019.
-
CMS changed the payment classification system for home health agencies in January 2020.
-
New metrics planned for Program for Evaluating Payment Patterns Electronic Report (PEPPER) will provide additional areas for auditing and monitoring.
-
Post-acute care providers should monitor coding, billing, and documentation to comply with these new CMS rules and regulations.
-
The PEPPER website (pepper.cbrpepper.org) includes additional information and offers assistance through the PEPPER Help Desk.