In a version of the appeals settlement process that it consummated with hospitals in 2014 and 2016, CMS on June 17 extended an offer to inpatient rehabilitation facilities (IRFs). CMS will pay IRFs 69% of the net payable amount for claims associated with appeals pending at all levels and, in some cases, 100% of the net payable amount. The process is available for appeals that were filed by Aug. 31, 2018, with the Medicare administrative contractor (MAC).
“The first thing I want to say is ‘Yay’ in capital letters,” says Jane Snecinski, president of Post Acute Advisors in Atlanta, Georgia. IRFs, which are licensed as acute-care beds and certified as rehab beds, have been seeking this option since CMS offered the settlement process to hospitals, especially because IRFs have been under intense scrutiny for years by Medicare auditors (“IRF Claim Denials Are Mounting; Auditors Use Coverage Guidelines, Eye Physician Notes,” RMC 26, no. 34), including recovery audit contractors and, more recently, in Targeted Probe and Educate.
IRFs are eligible for 100% of the net payable amount of their claims under either of two circumstances: when the claim was denied solely because “justification for group therapy was not documented in the medical record” or when the claim was denied based solely on patients not satisfying the threshold of therapy time in the absence of a more comprehensive medical necessity review.
“It’s a pretty fair settlement offer—69% for most appeals and then 100% for the other two categories, which is also a big win for IRFs,” says attorney Jessica Gustafson, with The Health Law Partners in Farmington Hills, Michigan. CMS paid hospitals 68% in the 2014 appeals settlement process and 66% in 2016.
“Some [IRFs] may opt to pursue the formal appeal process to get back 100% because they feel medical necessity is demonstrated, but after two to three years, their cash flow is impacted so significantly,” Snecinski says. So they will accept the settlement amount.
Gustafson advises IRFs to keep their eye on the Sept. 17, 2019, deadline for signing up, which requires submitting an “Expression of Interest” to CMS. The settlement process is different than the hospital version because it’s open to appeals pending at every level—the MAC, qualified independent contractor (QIC), administrative law judge (ALJ) and Medicare Appeals Council—although “as a practical matter, most of the appeals will be at the ALJ anyway” because the IRF settlement process is limited to appeals filed by Aug. 31, 2018, she says.
IRFs treat beneficiaries with serious diagnoses who need both medical care and rehab (physical, speech and occupational therapy). Medicare has six strict coverage guidelines for inpatient rehabilitation, and auditors may deny payment for the entire stay if IRFs fail to meet any of them. For example, patients must receive three hours of medically necessary therapy five days a week that they can truly benefit from and participate in. Medicare also accepts 15 hours of therapy a week averaged over seven days.
Claims Were Denied Over a Few Therapy Minutes
By offering 100% of the settlement amount in some cases, CMS is rectifying unfair denials stemming from therapy minutes at IRFs, Gustafson and Snecinski say.
Medicare auditors have been denying claims for the entire IRF stay when patients fall a few minutes short of the therapy hours identified in regulations, Snecinski says. A few skipped minutes may be inevitable in IRFs, where admission is only covered if patients require intensive rehab and have certain serious medical conditions (e.g., stroke), she explains. “I can’t tell you the number of denials received because patients missed only a few minutes of therapy. The criteria is they receive 15 hours of therapy over seven days, and sometimes patients received 14 hours and 45 minutes because of a medical issue and the whole stay was denied,” Snecinski says. Now CMS has clarified that if IRFs lost their entire payment for a medically necessary stay because of therapy minutes, they will receive 100% of their payment. “It demonstrates that the MACs and QICs may not have shared CMS’s understanding of medical necessity in inpatient rehab,” she contends.
Also, Medicare contractors at some point took the position that the minutes patients spent in group therapy should be discounted if the chart didn’t have an express statement explaining exactly why the patient was undergoing group instead of individual therapy, Gustafson says. “That caused a lot of denials because most providers hadn’t documented that way” and Medicare guidance hadn’t previously been interpreted as requiring them to, she says.
The IRF appeals settlement process is another avenue for reducing the enormous backlog of appeals pending at ALJs, Gustafson says. It’s one of several measures underway, including Settlement Conference Facilitation, which was recently expanded by the Office of Medicare Hearings and Appeals (“OMHA Expands Eligibility for Mediation of Medicare Appeals,” RMC 28, no. 22).
Contact Snecinski at jane.snecinski@postacuteadvisors.com and Gustafson at jgustafson@thehlp.com. Read about the settlement process at https://go.cms.gov/2IWsMhE. ✧
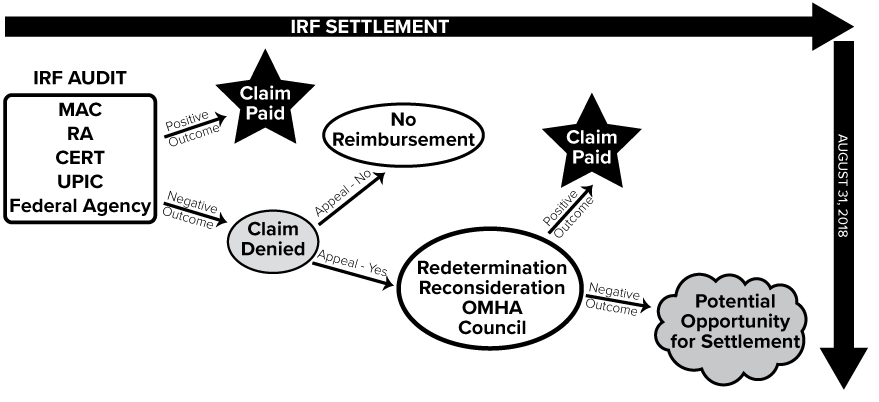
At a Glance: CMS’s New Appeals Settlement Option for IRFs
There’s a new settlement process for inpatient rehabilitation facilities (IRFs) with appeals of claim denials pending (see story, above). Here’s a depiction of how disputed claims may wind up there, says Jane Snecinski, president of Post Acute Advisors in Atlanta, Georgia. Contact her at jane.snecinski@postacuteadvisors.com.