This form helps hospitals elicit information from physicians to ensure surgery is performed in the correct status, said Ronald Hirsch, M.D., vice president of R1 RCM.[1] Contact him at rhirsch@r1rcm.com.
You Need to Know What Surgery Is Planned – Words and CPT Code!
Consent to Read: (please spell out complete surgery with no abbreviations, specify left and right)
_______________________________________________________________________________
_______________________________________________________________________________
Diagnosis:___________________________ ICD-10 Code(s): ______________________________
CPT Code(s) of planned procedure:______________, ______________, ______________
Insurance: ___________________________ Pre-Auth Number: ___________________________
Patient Status - Medicare Fee for Service Patient
_____ Day Surgery - plan discharge from recovery room
_____ Outpatient Extended Recovery - plan discharge next day, not high risk
_____ Inpatient Next Day Discharge - high-risk patient or surgery - risk factors must be outlined in documentation
_____ Inpatient - Inpatient Only List Surgery
_____ Inpatient - Expect 2+ Days In-Hospital Recovery
Discharge expected POD #2 or later - factors expected to extend in-hospital recovery must be outlined in documentation. Documentation not needed if LOS is always >2 days.
Patient Status – Other Insurers – Ordered Status Must Match Payer-Approved Status
_____ Day Surgery – plan discharge from recovery room
_____ Outpatient – Extended Recovery – plan discharge next day
_____ Inpatient
Anesthesia guidelines for medical necessity will be followed for all procedures with anesthetic.
Other Pre-admission Orders/Instructions: _____________________________________________
______________________________________________________________________________________
_____ Please initiate pre-procedure orders upon patient arrival.
Other Pre-procedure Orders/Instructions: ________________________________________
_________________________________________________________________________________
Physician Signature: __________________________ Staff Completing Form: ___________________
Date: ________________________
Give Your Doctors a Guide
Here’s a risk stratification and documentation tool for using the case-by-case exception to the two-midnight rule.
Medicare Total Joint Replacement Example of Wording
Admission as an inpatient is reasonable and necessary due to increased risk of surgery due to the factors indicated below or to the need for prolonged in-hospital or skilled post-acute care to improve the patient’s functional ability
Surgical Complexity
-
More complex intraoperative surgery anticipated due to _______________________________________________
Comorbid Conditions Increasing Perioperative Surgical Risk:
-
Poorly controlled diabetes. HbA1C=___________
-
Hypertension - either poorly controlled or requiring multiple medications for control
-
COPD/Asthma/OSA. Treated with (multi-select):
-
Home oxygen
-
Steroid dependent
-
Regularly scheduled inhalers/nebulizers
-
CPAP
-
Other _________________________
-
-
Cardiovascular Disease:
-
CAD
-
Stroke
-
Other _________________________
-
Anesthesia ASA Score of 3 or higher with factors indicated in anesthesia documentation
Note: ASA 3 is not automatically inpatient - must be supported with clinical factors documented
-
-
Anemia Hb<10
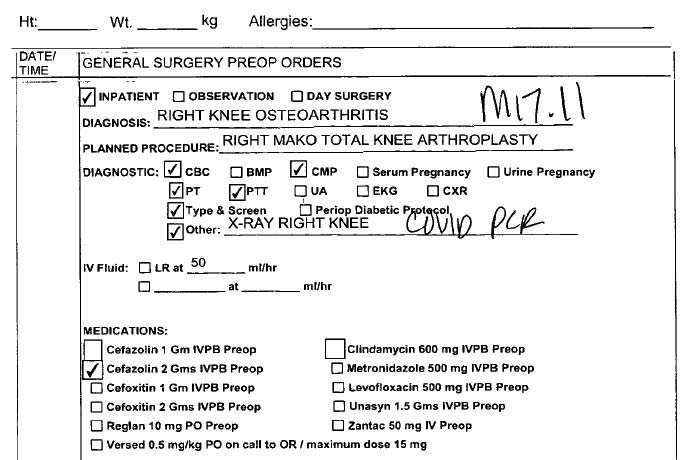
Don’t Do This!
Hospital scheduling forms should never offer the option of observation preoperatively, as shown below, Hirsch said.
Source: https://www.ronaldhirsch.com/total-joint-replacement.html