The No Surprises Act required that healthcare facilities and providers give good faith estimates (GFEs) to uninsured and self-pay patients starting January 1, 2022. To provide guidance about GFEs for healthcare facilities (which include Federally Qualified Health Centers (FQHCs), FQHC Look-Alikes (LALs), Tribal/Urban Indian Health Centers, Rural Health Clinics (RHCs), hospitals, hospital outpatient departments, critical access hospitals, and Title X Family Planning Clinics) and healthcare providers who serve uninsured and self-pay patients, the Centers for Medicare & Medicaid Services (CMS) produced the first of a series of FAQs on December 21, 2021.[1]
What is a GFE?
A GFE lists the expected charges for scheduled items or services that your clinical practice or facility will provide.[2] Because the GFE is based on information known at the time when it was created, it does not include any unknown or unexpected costs.
The purpose of a GFE is to help protect an uninsured or self-pay individual from unexpected healthcare charges; it allows individuals to compare prices for nonemergency healthcare goods or services. Examples of nonemergency ambulatory services are:
-
Behavioral healthcare
-
Dental and oral healthcare
-
Family planning services
-
Imaging services
-
Laboratory services
-
Outpatient physical, occupational, or speech therapy services
-
Prenatal and postpartum care
-
Primary healthcare
-
Vision services
Who needs to receive a GFE in ambulatory care settings?
To comply with federal requirements, healthcare facilities and ambulatory clinical practices must offer GFEs to two categories of individuals:
-
Those who have no health insurance coverage (defined as “uninsured”), or
-
Those who do have health insurance coverage but do not want to have a claim submitted to their insurer (defined as “self-pay”)
How HHS defines uninsured and self-pay individuals
The U.S. Department of Health and Human Services (HHS) defines the uninsured as individuals who do not have coverage for healthcare items or services under any of the following arrangements:
-
Commercial health coverage, such as a group health plan or a group or individual health insurance that a health insurance issuer offers
-
A federal employee health benefits plan (FEHBP)
-
A federal or federal/state healthcare program, such as Medicare, Medicaid, Medicare Advantage, or TRICARE
In August 2022, the U.S. Assistant Secretary for Planning and Evaluation, Office of Health Policy released its analysis of data about the number of uninsured individuals based on findings from the National Health Interview Survey.[3] While the rate of uninsurance varies by age and state of residence, the Office of Health Policy reported that approximately 8% of U.S. residents were uninsured.
HHS defines self-pay as individuals who have commercial health insurance or FEHBP coverage but who choose not to have a claim submitted to their insurer for the service. Two self-pay examples are:
-
A new patient contacts your behavioral health practice to book counseling services. The caller, who has employer-based health insurance, states they do not want their health plan billed. The individual should be given a GFE.
-
An established patient contacts your family practice, requesting testing for a possible sexually transmitted infection. The caller, covered by an FEHBP carrier, states they want to pay out of pocket for this service. This individual should receive a GFE.
Information about GFEs
Information about the availability of GFEs for uninsured or self-pay individuals must be:
-
Written clearly and understandably, and prominently displayed:
-
On the facility or practice’s website, which must be easily searchable from a public search engine
-
Onsite within the clinical practice’s office (for example, within the check-in or patient registration areas), and
-
Onsite in locations where scheduling occurs or questions are answered about the cost of items or services
-
-
Orally provided when scheduling an item or service or when questions about the cost of items or services occur, and
-
Made available in accessible formats and languages spoken by individuals considering or scheduling items or services
In developing your GFE communication strategy, check your website’s search engine to confirm that GFE content is accurate, accessible, and can be used by individuals with limited English proficiency and individuals with disabilities who may need auxiliary aids. Signage within your facility should be reevaluated periodically to confirm designated in-house contacts’ names and telephone numbers. Periodic “secret shopper” calls should be conducted to confirm that the GFE mailbox can accept new messages and monitor response turnaround times.
This information is necessary for established uninsured or self-pay patients, members of the public seeking care, and all staff members who triage incoming telephone calls, schedule appointments, or perform preregistration functions. Your GFE public education strategy should incorporate each component shown in Figure 1.
GFE content requirements
To comply with HHS requirements, a GFE must include the following components:[4]
-
The patient’s name and date of birth.
-
A description of the primary item or service in clear and understandable language (and, if applicable, the date the primary item or service is scheduled).
-
A list of items or services reasonably expected to be furnished for the primary item or service.
-
Applicable diagnosis codes, expected service codes, and expected charges associated with each listed item or service.
-
The name, National Provider Identifier, and Tax Identification Number of each provider or facility represented in the GFE, and the state and office of the facility’s location where the items are services are expected to be provided.
-
Lists of items or services that the provider or facility anticipates will require separate scheduling, which is anticipated to occur before or following the expected period of care for the primary item or service. (A disclaimer should state that separate GFEs will be issued upon scheduling or requesting the listed items or services.)
-
A disclaimer that there may be additional items or services that the provider or facility recommends as part of the course of care that must be scheduled or requested separately and are not included in the GFE.
-
A disclaimer that the information provided in the GFE is only an estimate and that actual items, services, or charges may differ.
-
A disclaimer that the individual has a right to initiate the patient–provider dispute resolution process if the actual billed charges are substantially in excess of the GFE.
-
“Substantially in excess” is defined as at least $400 more than the total amount of expected charges.
-
This disclaimer must include instructions about where an uninsured or self-pay individual can find information about how to initiate the patient–provider dispute resolution process and state that the initiation of the patient–provider dispute resolution process will not adversely affect the quality of healthcare services that are furnished.
-
HHS strongly encourages providers and facilities to include an email address and telephone number for a contact with the authority to represent the provider or facility in a billing dispute.
-
-
A disclaimer that a GFE is not a contract and does not require the uninsured or self-pay individual to obtain the items or services identified in the GFE.
GFEs for recurring services
When a provider or facility expects to furnish recurring items and services, then a single GFE may be issued rather than a GFE for each instance. Examples of recurring services are:
-
Intensive outpatient services for substance use treatment
-
A segment of outpatient behavioral health counseling sessions
-
A segment of outpatient physical therapy
-
Prenatal and postpartum care during a woman’s pregnancy
-
Prosthodontic services for dentures
A single GFE can be issued for a recurring primary service if:[5]
-
The GFE includes the expected scope of the recurring service
-
The scope must not exceed 12 months
-
-
The GFE includes the frequency, time frames, and total number of recurring services
A new GFE must be provided if additional recurrences are expected beyond 12 months.
The intersection of GFEs and sliding fee discount scale program requirements
An important consideration when designing a healthcare organization’s GFE template and communication strategy focuses on whether the organization is obliged to operate a sliding fee discount scale program. FQHCs—which receive funding under Section 330 of the Public Health Service Act—as well as FQHC LALs—which meet Section 330 requirements but do not receive Section 330 grant funds—must offer a sliding fee discount scale in compliance with requirements that are established by the Health Resources & Services Administration (HRSA) for the Health Center Program. Requirements for health centers’ sliding fee discount program are outlined in Chapter 9 of the Health Center Program Compliance Manual.[6]
HHS encourages sliding fee discount providers and facilities to include information about their sliding fee schedule and any other financial protections offered. Sliding fee discount providers and facilities have flexibility to determine how best to demonstrate the expected charges associated with each listed item or service and to determine what additional information to include, if any.
Principles of “plain writing”
Adopting plain writing when designing your GFE template can increase the likelihood that your patients will understand the intended message. The Plain Writing Act of 2010 defines plain writing as “clear, concise, well-organized, and follows other best practices appropriate to the subject or field and intended audience.”[7]
Plain language techniques can promote three aids to patients’ comprehension of their GFE, shown in Figure 2.
CMS developed a helpful reference you can use when editing your GFE communications for its own general communications. In its “Guidelines for effective writing,” CMS recommends the following practices:[8]
-
Keep sentences as brief as possible, preferably 20 words or less
-
At a maximum, paragraphs should be two or three sentences
-
Use active voice, not passive voice
-
Use common words and replace complex words with simple ones
-
Language to avoid:
-
Undefined abbreviations and acronyms
-
Using two different terms to mean the same thing (such as doctor, physician, provider), unless unavoidable by policy constraints or intentional for search engine optimization (such as health plan and health insurance)
-
Legal, technical, medical, or marketing jargon
-
Unnecessary intensifiers (such as very, much, or best)
-
Colloquialisms
-
Humor, which often does not translate well
-
Negative phrasing
-
Talking “at” your readers instead of “with” them
-
Avoid quoting laws and regulations unless necessary
-
Required methods for documenting the provision of a GFE
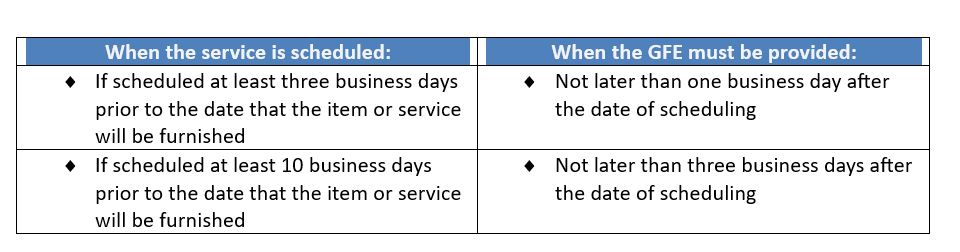
A GFE must be provided in written form, either on paper or electronically, based on the individual’s requested delivery method and within the required time frames (see Table 1). GFEs that are provided electronically must be provided in a manner that the individual can both save and print. A GFE must be provided and written using clear and understandable language and in a way the average individual can understand.
If the individual requests a GFE in a method other than on paper or electronically (such as by telephone or in-person), then the provider or facility may orally inform the individual of the information in the GFE. However, the GFE must also be issued in written form.
GFE timeline requirements
GFEs must be provided according to the timelines shown in Table 1. No GFE is required when a service is scheduled less than three business days in advance.
Required methods for providing and retaining GFE documents
A GFE must be retained in the patient’s electronic health record for six years so that a copy of any previously issued GFE is available upon the patient’s request. This must be produced not later than three business days after the date of the request. Retention of the GFE is crucial if the patient disputes the amount of their bill.
Independent resolution process
An uninsured or self-pay patient may dispute their bill if the amount exceeds their GFE by at least $400. HHS oversees an independent resolution process, known as the Patient-Provider Dispute Resolution (PPDR) process. Uninsured or self-pay patients are eligible to use the PPDR process if they meet all the following requirements:[9]
-
They scheduled and received the items or services on or after January 1, 2022.
-
They have a GFE from their provider.
-
They have a bill dated within the preceding 120 calendar days.
-
The difference between the GFE and the bill from any single provider or facility is at least $400.
Steps in the PPDR process
To start the PPDR process, HHS has outlined these steps for patients:
-
Submit an initiation notice through the online federal portal, or
-
Submit an initiation notice electronically, or
-
Submit a PPDR request through the mail if postmarked within 120 days of receiving the initial bill that has charges that are at least $400 more than expected based on the GFE
HHS strongly recommends submitting the initiation notice through the Federal IDR (independent dispute resolution) Portal to help ensure the request can be processed quickly and securely.
When submitting a PPDR, the patient must pay a $25 nonrefundable administrative fee when filing. If the outcome of the PPDR favors the patient, that amount will be deducted from the amount the patient owes the provider or facility.
Protections for patients during the PPDR process
During the PPDR determination period, patients are protected against debt collection. These protections are:
-
The bill for the disputed service cannot be turned over to a collection agency.
-
A threat cannot be made to turn the bill over to collection.
-
If the bill is already in collections, then the provider or facility must pause this action.
-
The provider or facility cannot collect late fees until the dispute process has ended.
Patients who have any issues with debt collection may submit a complaint to the Consumer Finance Protection Bureau by calling 855-411-2372.
Conclusion
The No Surprises Act required that healthcare facilities and providers give GFEs to uninsured and self-pay patients starting January 1, 2022. The purpose of a GFE is to help protect an uninsured or self-pay individual from unexpected health care charges.
Information about the availability of GFEs must be provided on the facility or practice’s website. Written information must also be provided within the clinical practice’s office and locations where scheduling occurs or questions are answered about costs.
HHS has outlined the mandatory components of a GFE, including a series of disclaimers. When a provider or facility expects to furnish recurring items and services, then a single GFE may be issued. If additional recurrences are expected beyond 12 months, then a new GFE must be issued.
HHS has established timelines for when GFEs must be issued. A GFE must be provided in written form, either on paper or electronically, based on the patient’s request. GFEs that are provided electronically must be provided in a manner that the individual can both save and print. A GFE must be retained for six years in the patient’s electronic health record. Retention of the GFE is necessary to produce a copy of any previously issued GFE within three business days of a request. Retention of the GFE is important if the patient decides to dispute the amount of their bill.
Takeaways
-
As the No Surprises Act requires, a good faith estimate (GFE) helps protect uninsured and self-pay individuals from unexpected charges for nonemergency health care.
-
The U.S. Office of Health Policy reported in August 2022 that approximately 8% of U.S. residents were uninsured.
-
In developing a GFE template, rely on “plain language” principles by avoiding heavy text, long sentences, and undefined acronyms.
-
GFEs must be retained for a period of six years.
-
If a patient’s bill exceeds their GFE by at least $400, they may file for an independent resolution process within 120 days of receipt.