Stewart M. Presser (stewartp@bluemark.net) is Senior Strategic Advisor and Bryan Exner (bryane@bluemark.net) is Chief Operating Officer with Bluemark in New Paltz, New York.
Due to the complexities of regulations and billing requirements, providers are faced with rapidly increasing volumes of audits and claim denials from all types of insurance carriers. Although initially only government payers, such as Medicare and Medicaid, were auditing and denying healthcare claims, now commercial insurance carriers also have instituted broad-based claim audits and regularly issue both technical and medical review denials. Today, hospitals and other caregivers are faced with a myriad of challenges to their claim dollars, including both prepayment and post-payment reviews.
With this barrage of audits and denials, providers need viable tools and processes to efficiently and effectively support the claim defense process and, ultimately, protect at-risk reimbursement dollars. At the foundation of an organization’s strategy, healthcare providers must establish a cross-functional audit and denial department dedicated to managing the impending wave of audit requests. A state-of-the-art technology solution to automate and facilitate the claim defense process across multiple departments is also a critical component for success.
Less than a decade ago, providers received an unmanageable volume of audit requests from payers, specifically Medicare audit contractors. At that time, manual processes and disparate, rudimentary systems—including simple spreadsheets and basic audit tracking software—were the only tools used to manage this process. It did not take long for providers to become overwhelmed with the volume. As a result, many audits turned into technical denials due to providers’ inability to submit initial record requests in a timely manner or manage the overall denial time frames. Over the years, the Centers for Medicare & Medicaid Services (CMS) realized that providers needed relief from these tremendously high request volumes.
This was a welcome change, but it still did not resolve the issue of audit and denials management or help ensure that providers never sustained a denial due to internal audit tracking issues. Other payers increased audits without regard to providers’ abilities to handle high volumes of requests. Providers are now faced with a whole new set of challenges, including:
-
How to respond to the now thousands of record requests from all payers on a regular basis,
-
Millions of dollars in prepay and post-pay reimbursement at risk, and
-
High rates of denials.
In its fiscal year 2016 Report to Congress, CMS stated:
Medicare FFS RACs collectively identified and corrected 380,229 claims with improper payments that resulted in $473.92 million in improper payments being adjusted. The total corrections identified include $404.46 million in overpayments collected and $69.46 million in underpayments repaid to providers. This represents a 7.5% increase from program corrections in FY 2015, which were $440.69 million. In FY 2016, the Medicare FFS Recovery Audit Program returned a net of $214.09 million to the Medicare Trust Funds. This represents a 50% increase from returned dollars in FY 2015, which were $141.87 million. These savings take into consideration the costs of the program, including contingency fees, administrative costs, and amounts overturned on appeal.[1]
State Medicaid and private insurance payers historically look to Medicare results to hone their audits on providers, which leads to increased audit volumes. The assumption is, if the provider codes incorrectly for Medicare, they will likely have a certain coding error on all payer claims. The Health and Human Services Office of the Inspector General (OIG) consistently monitors federal agency audit results, and then embarks on their own audits, oftentimes duplicating what other federal audits have already done. Unfortunately, the OIG is not exempt from duplicating what other Medicare audits have done, so it’s possible that providers can experience duplicate audits by the OIG.
This increased volume of audit activity will stress current processes in place and reveal workflow gaps and inefficiencies. Driving many of these challenges for providers is the lack of integration between existing audit tracking software and the systems used for key activities, such as billing, medical records and financial reporting. This disconnect can result in highly manual processes and leave providers at risk for data quality issues. This also makes it difficult to manage audit support activities among department team members, both across the organization and with third-party support vendors, all of which affects the ability to provide timely responses to record requests and meet strict appeal deadlines. Additionally, specific technical challenges include tracking high-volume denials, lack of system integration across platforms, and the need for manual intervention throughout the process.
How we got here: A brief history of audits
Before moving forward, let’s take a moment to look back at the history of audits and denials to help understand where we are today. In 2006, Congress authorized the Centers for Medicare & Medicaid Services (CMS) to initiate the Recovery Audit Contractor (RAC, now RA) program in the form of a demonstration in three states: New York, Florida, and California. The success of this demonstration, specifically in terms of how much the audit contractors denied claims and returned funds to the Medicare trust fund, led Congress to expand the RAC program nationwide in 2010. Most providers were not prepared for the onslaught of medical record requests, known as additional documentation requests (ADRs). They were also challenged with short time frames established by CMS to submit the records and sustained denials simply because they were not able to respond and submit records on time. Many providers lost their initial claim payment due to what many consider overzealous audit contractors denying as many claims as possible. Simply stated, these contractors were paid by CMS on a contingency fee basis—meaning the more dollars they denied and “recovered,” the higher the fees they collected. Under Medicare rules, providers are permitted to appeal any denials, and many were successful in recovering previously lost funds. Over a short period of time, the Medicare appeals process became overwhelmed with provider claims at all levels, especially at the third level known as the Administrative Law Judge level. Further compounding the appeal process, providers were faced with strict time frames for the submission of appeals, and many were denied due to tardiness in filing.
Of course, Medicare audits were not new to providers in 2010. The Medicare Administrative Contractors (MACs) were in the audit arena well before the RAs came on the scene, but the rules of audits for them were not as tightly defined as with the RAs. In addition, the Medicare Comprehensive Error Rate Testing (CERT) program audited hospital claims but not to the same level as the RAs. CMS initiated the CERT program to calculate the Medicare Fee-for-Service (FFS) improper payment rate. Each year, CERT evaluates a statistically valid stratified random sample of claims to determine if they were paid properly under Medicare coverage, coding, and billing rules.[2] State Medicaid programs also audit provider claims and, under the Affordable Care Act (ACA), states were required to set up RA programs but did not necessarily have to follow Medicare’s rules established by CMS.
Lastly, commercial insurance carriers became more aggressive with claim audits, mainly with medical necessity audits and coding audits on all providers.
Convergence of audit and denials management
In the healthcare insurance arena, an audit is generally defined as a review of either:
-
A claim submitted for payment, in which case the provider’s dollars are held up pending the outcome of the pre-pay audit; or
-
A previously paid claim, meaning the provider’s payment is in jeopardy if the audit turns into a denial.
A denial is generally defined as the audit result. This will either:
-
Start the process of provider payment recoupment; or
-
In the case of Medicare, the provider can stop the clock and initiate an appeal but could be subject to interest payment if the appeal is not successful.
Historically, providers would manage these two distinct processes in separate systems with separate teams. Over the past few years, however, the process to manage audits and denials has become more similar than different. For example, denials have expanded to include a large number of claims for the same suspected over coding, which leads to payments of a higher weighted diagnosis-related group (DRG). These types of audits require a multidisciplined approach involving the health information management (HIM) team’s coding experts to determine if the DRG assigned was correct and research the appropriate coding guidelines to support their opinion so the information can be included in the provider’s appeal. This cannot effectively be handled by just the finance team or the compliance group.
-
Audits have also expanded to include more types of denials, including prepayment and post-payment. How should the provider record a prepayment audit if there hasn’t been a payment? They do not want to continue to follow up with the payer regarding when the payment will be received if the claim is under audit, so the receivable needs to be flagged pending outcome of the audit. Most providers act on only post-payment audits; however, prepayment audits are just as important to be followed in the event the claim is denied prior to payment. Appeals on prepaid denials are just as important as on post-payment denials.
-
Denials essentially follow the same process as an audit. Both include requests for documents and document submission and have appeal processes and time frames.
-
Provider teams tasked with addressing audits are typically focused on two things: reviewing the audit request and providing the audit agency with the requested documentation to support the original claim. Although this is technically correct and necessary, the long-range goal is often overlooked: total management of the audit and the possible future denial of previously paid claims.
Large providers should focus on a system-wide approach to managing this process. An audit and denials management system must involve all departments within the provider to ensure that audit items and the ability to appeal denials are not lost. Providers with several hospitals in a system need to coordinate activity on a corporate level so that all the system’s hospitals are addressing audit and denials management in the same way. The ideal approach is to have one department ultimately responsible for the management of the process. For example, the compliance officer and staff may want to take on this responsibility and involve the appropriate departments to support their respective areas:
-
HIM to process the request for a clinic record,
-
Case management to review audits pertaining to type of admission and/or length of stay audits, and
-
Revenue cycle staff to authenticate the audit and the initial payment made to the health system.
Once the audit results are received, the compliance staff would enter the results in the denials management system and determine if appealing the decision is appropriate.
The last part of audit and denials management is to keep senior leadership informed and up to date regarding results and outcomes. The audit and denials management system should be able to produce a plethora of reports that the chief financial officer (CFO) and other senior staff can use to make decisions with respect to the causes of audit denials. What are the trends? Is there a coding issue, which means further education in the HIM department? Is there a clinic issue, which necessitates physician support? The CFO will also rely on the audit and appeal results to determine if additional financial reserves are need.
Identifying the right solution
With this as the background to healthcare claim audits and denials, it is easy to see why it is absolutely critical for providers to establish a clearly defined audit management process—one that ensures they meet all of the auditor’s requirements for documentation submissions and controls their appeal rights. In a multi-facility healthcare organization, an audit management solution is the foundation for successfully managing this process cross-functionally throughout the organization.
Many departments are involved with the audit and appeals process, and they must work in concert to meet all audit requirements and deadlines. This may include medical records, case management, finance, revenue cycle, and compliance. By working closely together and maintaining a high degree of communication, these departments can ultimately ensure technical denials that cannot be appealed are eliminated.
A technology solution plays a key role in the audit and denials management process and provides a strong foundation for evolution and improvement. The most effective solutions enable an integrated, streamlined approach; seamless data sharing; and automated workflows. Identifying a scalable solution is also critical to support organizational expansion and onboarding new facilities. Ensuring an easy and painless transition for the end-users is also essential for success.
Technical requirements to consider when evaluating new solutions:
-
Integration with current systems is essential
-
Access for third-party vendor partners
-
Real-time appeals tracking
-
Electronic repository for all correspondence
-
Financial reporting
Beyond the technical requirements of a new solution, providers should look for a solutions expert with deep industry knowledge and a thorough understanding of the complexity of audits and denials. This will enable your vendor partner to facilitate the continued evolution of established processes by looking ahead to identify potential issues and impacts; proactively making appropriate system enhancements; and, ultimately, driving further efficiencies.
System design and implementation
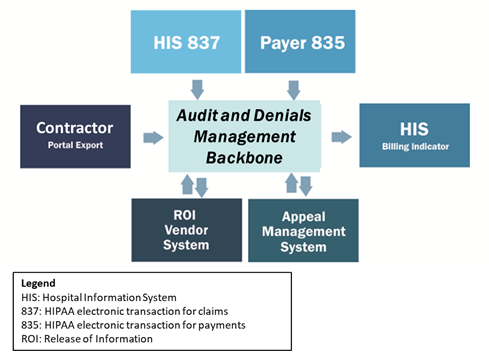
The first step in any implementation process is for the provider to clearly define business needs, because these will direct the design of the solution. Audit management backbone systems provide an ideal foundation (see Figure 1), but implementation needs to satisfy the specific requirements of the organization to be considered a success. In many cases, this means customizing certain aspects of the solution, typically accomplished through close collaboration among the key stakeholders and project team.
Mature and market-tested audit management solutions are an excellent starting point for many reasons. Typically they have existing interface methods in place that are paramount in satisfying the oftentimes disparate interface requirements. These existing interface methods can be further leveraged to implement the specified needs of the client. Figure 1 illustrates an overall audit and denials management system design at the very highest level. This designed system is built around the audit management backbone that coordinates all data sharing and system traffic.
The implementation process can be a challenge and requires strong project management to ensure all involved parties, both internal provider stakeholders and third-party vendors, are aligned and that the systems used by each will be able to communicate seamlessly through the audit management backbone. To ensure success, dedicated project managers need to be required of all vendors, plus the provider must designate an internal project owner to act as the ultimate project lead. Standard project management techniques should be used throughout the implementation process to provide a strong framework and invaluable support for the complicated technical nature of the implementation and the number of parties involved. Written plans, excellent technical interface documents, status calls, and strong communication around issues are among the core tools that established a strong foundation for a project’s success.
Expected results
Certainly many variables must be considered when evaluating the success of implementing a backbone audit and denials management platform. When done effectively, providers can expect the following results.
A high degree of automation
With manual processes and disparate tools, providers often have to rely on valuable clinical resources to complete data entry tasks instead of working on the specifics of the appeal or denial. Non-integrated systems can also require significant “monitoring” of billing systems and information, because data feeds of claims and remittances are not automated.
Standardized enterprise-wide workflows
In multifacility health systems, all facilities will have standardized workflows across the enterprise. A strong backbone audit system with technical capability and understanding of the audit and denials process is necessary for this to happen.
Real-time work lists available anytime to end users and managers
This will help to meet deadlines, allow audit case managers to prioritize the team’s work, and enable the reassignment of tasks as needed. Providers should also expect to reduce time spent creating and reviewing work lists.
Enhanced data integrity
Maybe the most important aspect of a backbone audit management solution is having greater confidence in data reported to the organization’s finance department and other key leadership stakeholders. Providers will experience a reduction in time spent running reports and validating data with financial reporting teams, as well as reduced resources required to execute reporting requirements. Ultimately, enhanced data integrity is the result of the increased automation.
Takeaways
-
Create a single process and unified technology platform for both audit response and denials management.
-
Departments involved, including medical records, case management, finance, revenue cycle, and compliance must work in concert to ensure time-sensitive deadlines are met.
-
Tightly integrated systems can reduce manual processes, eliminate errors, and increase automation.
-
Tracking audit and denial activity across all payers can hold contractors accountable to CMS regulations regarding permissible activity.
-
Audit appeal and denial results can be used in future contract negotiations. Demonstrated claim defense success can be leveraged into more favorable audit and denial terms.