
Calvin London (calvin@thecomplianceconcierge.com) is the Founder and Principal Consultant of The Compliance Concierge.
Risk management plans (RMPs) for pharmaceutical products originated as regulatory responses to public concerns that pharmaceutical medications were being approved too early. As a result, known problems from using the medication did not become apparent until after introduction into the marketplace.
RMPs are not designed to mitigate adverse events or their reporting. Rather, they are required by some regulatory agencies to specifically manage known risks associated with the use of a drug. Although these go by different names and require differences in design, approval, and operation, they all have a common core element—compliance.
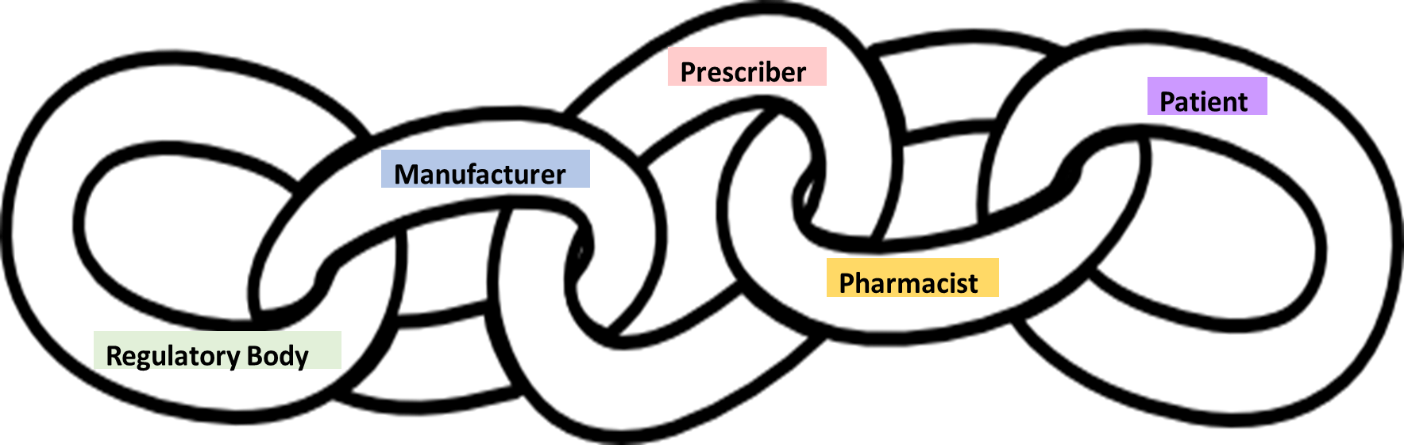
In all medication regimes, there is an unspoken requirement for compliance. While this is often assumed to only be relevant to the manufacturer (also known as the sponsor), RMPs provide an opportunity to look at the broader requirements for compliance at all steps of the process, from drug registration through to patient use. The operation of an RMP is a shared responsibility among the regulatory body, the manufacturer, prescriber, pharmacist, and the patient. This can be viewed as a chain of responsibility, as shown in Figure 1.
Prescribers and pharmacists both uphold the principles of the RMP. However, as described later, the overall success of the RMP is just as dependent on the individual patient’s sense of responsibility to be compliant. A breakdown in compliance in any of the links—manufacturer, prescriber, pharmacist, or patient—can have significant effects on the effectiveness of the RMP.
Regulatory body
The regulatory body mandates the RMP requirements that the manufacturer must satisfy to maintain compliance with their product registration. In most situations, once this is done, the regulatory body then assumes the manufacturer will execute the RMP and be held responsible for its compliance. As the first link in the chain, they do not have a compliance responsibility as such but do have high expectations of the compliance of the other links to uphold the principles of patient safety.
Manufacturer/sponsor
In the United States, a Risk Evaluation and Mitigation Strategy (REMS) is required by the U.S. Food and Drug Administration for certain medications with serious safety concerns to help ensure the benefits of the medication outweigh its risks.[1] This is the US version of an RMP, and currently, there are some 63 approved REMS.[2] Programs with a similar intent are also required in other regulated markets. For example, the European Medicines Agency requires RMPs for marketing authorizations,[3] as does the Therapeutic Goods Administration in Australia.[4]
In most cases, the nature and extent of the RMP will depend on a combination of special requirements such as testing prior to dispense or use; restricted access to the drug; education of prescribers, pharmacists, and/or patients; and ongoing monitoring of compliance.
Clozapine, for example, which is indicated for the treatment of severely ill patients with schizophrenia who fail to respond adequately to standard antipsychotic treatment, has caused severe neutropenia (defined as an absolute neutrophil count of less than 500/μL).[5] Severe neutropenia can lead to serious infection and death. As such, the RMP for Clozapine products requires the establishment of a minimum level of neutropenic activity prior to use and baseline monitoring during use.[6] Companies that market clozapine provide a database for the monitoring of these results and information related to the use of the drug for physicians to educate patients.
Other examples, and perhaps one of the best known RMPs among the pharmaceutical community, are for the use of Isotretinoin, indicated for the treatment of severe recalcitrant nodular acne, and the immunomodulatory drugs—thalidomide, lenalidomide, and pomalidomide—indicated primarily for the treatment of multiple myeloma. These are not only the most detailed and exacting RMPs, but were also made for the drugs that lead to the global use of RMPs. Readers may be familiar with the issues that resulted from the use of Thalidomide in the 1950s, when the drug was first marketed for morning sickness.[7] Enhanced regulatory compliance, particularly in Australia, Canada, and the United States, was implemented to prevent the issues associated with the development of fetal abnormalities, including amelia (congenital absence of limbs), when Thalidomide was brought back onto the market.[8]
Immunomodulatory drug RMPs call for three areas of manufacturer or drug sponsor compliance: (i) controlled access to the product; (ii) educating prescribers, pharmacists, and patients; and (iii) ongoing compliance monitoring.[9] In short, the requirements of these RMPs include:
-
Registration of prescribers, pharmacists, and patients into a formal program with appropriate consents;
-
Extensive education of prescribers, pharmacists, and patients to qualify for prescribing, dispensing, or using of the drug;
-
Limited supply of drug product to patients, especially those that are considered high risk, as well as women of child-bearing potential (WCBP);
-
Monthly pregnancy testing of WCBP to ensure they are not pregnant while undergoing treatment; and
-
Use of approved contraception by all patients while undergoing treatment.
Additional information for those interested can be found in different reviews.[10]
The compliance responsibility of the sponsor is to establish and maintain a robust RMP and to monitor its performance. As discussed in later sections, the sponsor cannot take total responsibility for the compliance (or lack of) for the other links in the chain. They do, however, need to encase their RMP in a suite of policies and procedures that account for and deal with noncompliance when it occurs.
Prescriber
The role of the prescriber in an RMP is no different from their responsibilities for any form of drug prescription. As RMPs are put in place to manage known side effects of a drug, the prescriber plays a key role in educating the patient. In order to do this successfully, they themselves must be compliant with the boundaries of the RMP. Failure on behalf of the prescriber to effectively gain the appropriate consent from a patient and to follow through with sound education can very quickly result in a failure of the entire process and expose significant risks for patient safety.
For example, if an RMP requires the use of specific, effective forms of contraception, and a prescriber fails to communicate this to the patient, this could easily result in a pregnancy-associated birth defect. Similarly, prescribing more than the allocated amount of permitted drug may be captured by a robust monitoring program, but only if it can track this aspect of prescribing habits.
In most RMPs, the prescriber is the first line of defense with the patient. With the heightening of data privacy requirements, particularly in Europe and some Asia-Pacific countries, only the prescriber has the contact details of the patient. It follows that their role in maintaining the intent of the RMP (i.e., to provide added patient safety) is heavily dependent on their own understanding of the requirements through training and education, as well as their ongoing compliance with the requirements.
Pharmacist
In the chain of responsibility, the pharmacist is the last protective link before the medication is given to the patient. RMPs test the integrity and ethics of pharmacists to do the right thing and abide by the requirements of the RMP.
As an example, some RMPs require the pharmacist to obtain a verification (approval) number before they issue the scripted medicine to the patient. Compensation for this additional activity or time spent in dispensing is not always commensurate with the effort and provides opportunities for pharmacists to take shortcuts unless the RMP program put in place by the manufacturer for monitoring compliance is robust. Programs that require ongoing monitoring, such as those that relate to monthly negative pregnancy tests, require the pharmacist to collect the evidence. Similarly, the pharmacist is the checkpoint to ensure that maximum limits of dispensing for the drug are respected.
On top of these responsibilities, the pharmacist must also ensure that the documentation trail is accurate and complete. As a minimum requirement, there is usually a patient card to be signed. At the other end of the spectrum, the pharmacist must enter data into a database, wait for the approval, and then write the approval number on the script. Although not common outside of North America, pharmacies and pharmacists are subject to routine audits to assess their levels of ongoing compliance.
Patient
When we think about the compliance of medication and RMPs in particular, the focus is usually on the company, to a lesser extent the prescriber, and sometimes the pharmacist. As reinforced throughout this article, it is a chain of responsibility, with the final link being the patient. The whole process of protection can be easily undone if patients do not comply with the program’s requirements.
An article on medication noncompliance lists data from the World Health Organization, according to which “approximately 125,000 people with treatable ailments die each year in the United States because they do not take their medication properly,” “about 50% of prescriptions filled for chronic diseases in developed countries are not taken correctly, and as many as 40% of patients do not adhere to their treatment regimens.”[11]
The distinction between medication compliance (the act of taking medication on schedule or taking medication as prescribed to achieve the desired health benefit) and medication adherence (patients sticking to a therapeutic regimen) is an important one that also takes into consideration social and environmental influences.[12] RMPs largely focus on adherence; compliance is still largely up to the patient.
From my experience, patients on RMPs tend to take their medication appropriately. This is especially so when the prescriber has adequately defined the chronic nature of their disease and the need for controlled medication (i.e., they have been compliant), and the pharmacist has been compliant and delivered the appropriate medication with an adequate explanation of how to take the medication. The RMP structure aims to prevent noncompliance at the prescriber and pharmacist level. However, it cannot control or monitor all aspects of successful medication, especially at the patient level. Once the medication has been dispensed, the best that an RMP can do is detect noncompliance and provide a framework for corrective actions.
For example, with the immunomodulatory drugs that require pregnancy testing prior to each prescription cycle, the drug should not be dispensed without a pregnancy test for WCBP patients. However, one of the most important aspects of the immunomodulatory drug RMPs is the need to use two forms of effective contraception to prevent the patient or patient’s sexual partner from becoming pregnant. Whether a male patient is compliant with one or more partners cannot be directly controlled and relies on the ethical approach of the patient to their treatment.
Compliance in the ultimate program
The success of RMPs is dependent on the sequential compliance of all its moving parts. The manufacturer of the plan must provide the infrastructure to maximize success and provide ongoing monitoring to measure compliance, much like any compliance program. The prescriber has a responsibility to provide the correct guidance and education to the patient to ensure they are equipped to conduct their part in the overall compliance. The pharmacist is also responsible for affecting the day-to-day management and is the primary liaison with the patient. Their responsibility as the last part of the controlled plan is to also ensure that the patient has a clear understanding of their responsibility.
I have had ten years of experience with the implementation and management of RMP programs of varying complexity and accompanying compliance requirements. Like many regulatory processes, regulators err on the side of caution when it comes to patient compliance, and in their infancy, many compliance requirements are seen by the different users as unnecessary. This is reflected in the most common types of noncompliance that occur in RMPs—documentation omissions. Prescribers and pharmacists that have the perception that the RMP is unnecessary—or certainly some elements of the RMP—are less likely to pay attention to the details leading to noncompliance events. RMPs must include effective monitoring to detect noncompliance at the time it occurs, otherwise their correction becomes retrospective, potentially compromising patient safety.
The ultimate success of the RMP has to be measured in how successfully it manages and/or prevents the known risk(s) that it was put in place to prevent. To date, most have been largely successful. For example, with Clozapine, prevention of the development of severe neutropenia, and with immunomodulatory drugs, the prevention of pregnancy while patients are on the medication. As we become more protective of patient data privacy, and as RMPs mature, it is possible that the structure of RMPs will become more simplistic and less arduous to monitor. Ultimately, the best RMP with the most compliant prescribers and pharmacists cannot negate the actions of the patients—the most difficult link in the chain of responsibility to control.
Conclusion
RMPs require a commitment by all participants—the patient, the pharmacist, the prescriber, and the manufacturer. When one of the links breaks, the potential for the whole plan and the intent (i.e., patient well-being and safety) are compromised. As with many structured programs for managing and monitoring compliance, the end result is heavily dependent on each link being compliant, and the overall success of the plan is the sum of each of its parts.
Takeaways
-
Risk management plans (RMPs), designed to manage known risks from drugs during their use, have compliance as a core element.
-
RMPs provide an example where their success is dependent on a number of combined compliance efforts—a chain of responsibility.
-
The responsibility of the manufacturer is to establish and monitor the RMP, but prescribers and pharmacists also have compliance responsibilities.
-
RMPs must include effective monitoring to detect noncompliance at the time it occurs; otherwise, their correction becomes retrospective, potentially compromising patient safety.
-
As with many structured programs for managing and monitoring compliance, the end result is heavily dependent on each link being compliant.