Table of Contents
After Prime Healthcare Services acquired Roxborough Memorial Hospital in Philadelphia, physicians there allegedly were pressed to add complications or comorbidities (CCs) to their Medicare patients’ medical records. Clinical documentation specialists (CDSs) employed by Prime, a California-based hospital chain, gave physicians leading queries so they could document higher-paying MS-DRGs, according to a False Claims Act complaint. If physicians didn’t play ball, they allegedly were suspended until they got with the game.
The alleged strategy appeared to work, according to the complaint. For example, the number of syncope cases (MS-DRG 312) dropped 17% in 2013, the year after the hospital acquisition, while cases of cranial and peripheral nerve disorders (MS-DRG 074), which is similar to syncope but pays $1,000 more, rose 30%, the complaint alleged. But it wasn’t just a matter of money because the complaint alleged that patients were treated as if they had the more serious conditions.
Now Prime Healthcare Services and its CEO, Prem Reddy, M.D., have agreed to pay $1.25 million to settle allegations that Roxborough Memorial Hospital and another Prime hospital—Lower Bucks Hospital in Bristol—submitted false claims to Medicare by upcoding diagnoses and admitting inpatients who only required outpatient care, the U.S. Attorney’s Office for the Eastern District of Pennsylvania said Feb. 15.
The settlement came down about seven months after Prime and Reddy paid $65 million to resolve a separate false claims lawsuit in California, which was set in motion by a whistleblower. The Department of Justice alleged 10 of its hospitals billed for inpatient admissions that should have been outpatient or observation services from 2006 to 2013. Reddy had to personally pay $3.25 million of the settlement amount. (“Prime Healthcare, CEO Settle FCA Case for $65M Over Admissions; Accountability Expands,” RMC 27, no. 29)
In a statement on the Pennsylvania settlement, Prime Healthcare said it “contains no finding of improper conduct or wrongdoing, and Prime Healthcare’s record of clinical quality care was never in question. Prime Healthcare is committed to defending patients’ rights and physicians’ decisions in the delivery of excellent care.”
This complaint was set in motion by three whistleblowers: Roxborough Memorial Hospital employees Melanie Dudek and Angela Rodriguez, and Stop Community Hospital Upcoding LLC, a corporation that “was formed for the purpose of bringing this action,” the complaint states. The person who signed the settlement on behalf of Stop Community Hospital Upcoding is John Mininno with the NHCA Group. According to DOJ, the NHCA Group is made up of limited liability companies that were formed by investors and former Wall Street investment bankers. NHCA Group is the whistleblower behind 11 false claims lawsuits against pharmaceutical companies, which DOJ asked federal judges to dismiss in December 2018 (“DOJ Moves to Dismiss 11 FCA Suits With Same Relators Alleging Nurse Educators Are Kickbacks,” RMC 27, no. 45).
The whistleblowers in the Prime case allege the trouble at the two Pennsylvania hospitals began after Prime bought them in 2012 and installed a CDS team. Physicians allegedly were prohibited from diagnosing patients with conditions that generated lower Medicare reimbursement. “Prime physicians are functionally required, instead, to diagnose patients with similar—but reimbursable at a higher level—conditions,” the complaint alleged.
CDSs generally help physicians improve their documentation and code assignment. At the two Prime hospitals, however, CDSs used concurrent review to pressure physicians to change diagnoses in the service of greater reimbursement, according to the complaint. When they would determine a diagnosis was similar to a higher-paying diagnosis, CDSs queried the physicians. Physicians then had to “provide a post-hoc justification for the diagnosis and provide additional information in the patient’s chart,” the complaint alleged.
AHIMA Updated Query Guidance in 2019
Physician queries are requests, usually from coders or clinical documentation specialists, for clarification of documentation to ensure correct code assignment (see example below). They should not lead physicians to a diagnosis, according to a 2019 practice brief from the American Health Information Management Association (AHIMA) and the Association of Clinical Documentation Improvement Specialists, which updated a 2016 AHIMA version. “Avoid queries that: Fail to include clinical indicators that justify the query or justify the choices provided within a multiple-choice format; Encourage the provider to a specific diagnosis or procedure; Indicate the impact on reimbursement, payment methodology, or quality metrics,” the practice brief states.
At Roxborough Memorial Hospital, physicians who didn’t respond to queries in 14 days were suspended until they complied, according to the complaint. This had a powerful effect on other physicians, who worried about their job security. After the Prime CDS procedures were adopted, “the number of queries that the CDS teams have needed to perform have declined strikingly.” And the MS-DRGs changed accordingly, the complaint alleged. For example, the year after Prime acquired Roxborough Memorial Hospital, its billing for miscellaneous disorders of nutrition, metabolism, fluids with electrolytes without major CC, which pays $3,978, dropped 35%, while billing for the same MS-DRG with major CCs, which pays $6,377, increased 53%.
The upcoding allegedly wasn’t confined to paper. Patients were receiving treatment for more serious conditions than justified based on their actual conditions, and as a result, were “routinely given stronger medications and are forced to undergo unnecessary procedures for the sole purpose of ensuring the treatment provided matches the DRG code billed to Medicare,” the complaint alleged.
DOJ alleged the upcoding persisted from the time the hospitals were acquired until Dec. 31, 2014.
The settlement also resolves allegations that the two hospitals admitted inpatients who could have received observation or outpatient services from the time the hospitals were purchased by Prime through Sept. 30, 2013.
Reimbursement Is ‘Not the Goal’ of CDSs
When they’re put to good use and practicing ethically, CDSs help physicians “accurately represent how sick and complex a patient is,” according to clinical documentation and coding consultant Erica Remer, M.D., who thinks CDSs should be called CDISs, for clinical documentation integrity specialists. While their efforts almost always help hospitals increase reimbursement, “that’s not our goal,” she says. Physicians have an obligation to accurately portray the patient’s condition in the documentation and coding.
Suppose the patient has altered mental status (AMS), “which indicates something bad is happening to the patient, but that verbiage does not get captured with a risk adjusting code”—a CC or major CC (MCC)—Remer says. If the patient’s AMS is a manifestation of acute encephalopathy, it’s an MCC, assuming it’s documented and coded properly. “But you don’t want doctors to call every patient with AMS, such as transient confusion, acute encephalopathy,” Remer says. “You don’t want to indiscriminately risk adjust.” Capturing secondary diagnoses also affects quality metrics, including report cards and hierarchical condition categories used by Medicare Advantage plans.
Physicians and hospitals find themselves caught between CDSs, whose work product often increases the capture of CCs and MCCs, and clinical-validation auditors who deny CCs or MCCs, Remer says. “We are spending a lot of time fighting [denials] when we shouldn’t have to,” she says. Ideally, the CDS will help physicians document accurate diagnoses in a codable format that’s unassailable. “We need good clinical education by the CDSs.”
In its statement, Prime Healthcare said it settled the false claims lawsuit because it decided “it was in the best interest of its patients, independent physicians, and employees to resolve this matter and continue the important work of ensuring community access to quality care.”
Contact Remer at icd10md@outlook.com. Visit http://bit.ly/2GD2e66. ✧
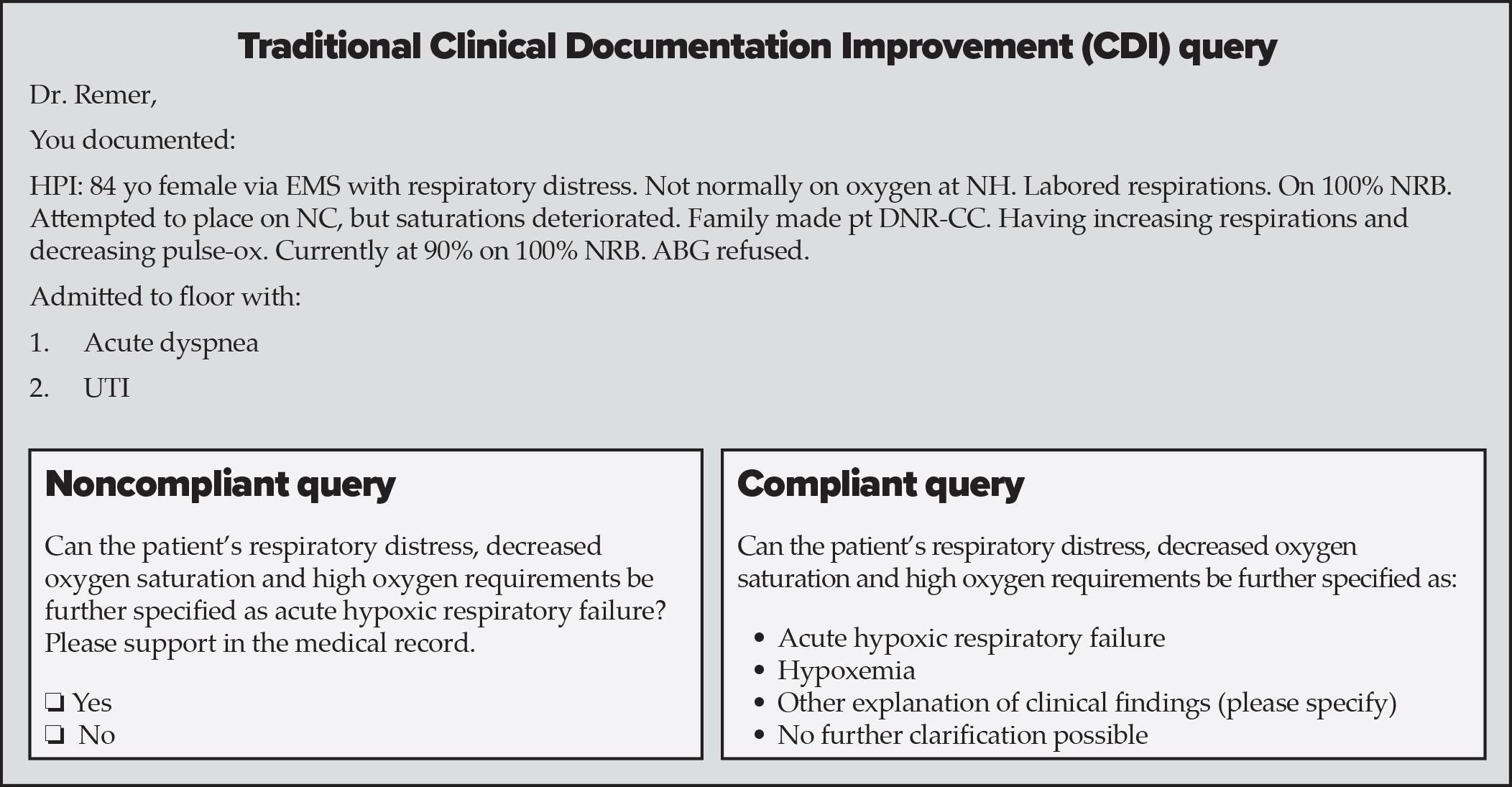
Physician Queries: An Example of the Right and Wrong Ways to Go
Here’s an example of a compliant and noncompliant query from a clinical documentation improvement specialist. It was provided by coding and clinical documentation improvement consultant Erica Remer, M.D. Contact her at icd10md@outlook.com.