


Medicaid program integrity has never been under as much scrutiny as it is right now under states’ unwinding of autoenrollment imperatives of the Public Health Emergency.
Stakeholders use many tools to minimize negative impacts of noncompliance or inaccurate compliance with regulations, policies, and guidelines per redeterminations so that Medicaid and the Children’s Health Insurance Program (CHIP) work as intended and for those who need it. It has widely been reported that roughly 10 million beneficiaries will no longer be Medicaid-eligible from the swells of the pandemic, yet the U.S. Department of Health & Human Services estimates that roughly 6.8 million will lose Medicaid coverage despite being eligible.[1]
One tool stakeholders can use to identify negative impacts of the massive administrative undertaking and to mitigate effects of current and new Administration policies in response to the COVID-19 pandemic is the Centers for Medicare & Medicaid Services’ (CMS) Payment Error Rate Measurement (PERM) data. CMS has been using PERM since 2007 to help states improve accuracy of Medicaid and CHIP payments.
What is PERM
Medicaid and CHIP are among the states’ largest expenditures. Combined federal and state contributions in fiscal year 2021 (recently available) totaled $734 billion for Medicaid and $22 billion for CHIP.[2]
With programs of this size, even small error rates can amount to billions of dollars in improper payments. Moreover, given the number of players involved in the program—states, hospital and health systems, professional providers, managed care entities, local health entities, patient stakeholder groups, and more—and the fact that state programs vary from one another, the programs inherently result in administrative errors and monetary losses due to those errors.
PERM helps reduce the number of administrative deficiencies and monetary losses in each state. Uniquely, 2022 is only the second year since program inception that CMS has reported publicly at the state level.[3] This data can be useful now.
Specifically, PERM produces statistically valid estimates of the amount of improper payments and monetary losses for each program every year. PERM’s methodologies are complicated: Briefly, CMS contractors review a sample of claims paid in 17 states (including the District of Columbia) to assess errors in three areas:
-
Eligibility
-
Fee for service (FFS)
-
Managed care
FFS claims are reviewed for adherence to federal regulations and state policies, and they undergo a medical record review. Managed care payments are subject only to the data processing review of adherence to federal regulations and state policies. The variance in methodologies consistently yields higher FFS improper payment rates than managed care rates: Current Medicaid FFS error rates are 10.42% versus 0.03% for managed care Medicaid error rates.[4]
CMS rolls the results from the current year plus the results of the two previous years from the other two 17-state cycles to a national improper payment rate. As previously cited, rates are also calculated for each state; states must submit corrective action plans to address the root causes of improper payments identified in their sample of claims.
2022 PERM rates
CMS’ 2022 published national improper payment estimates were 15.6% for Medicaid, representing $80.6 billion, and 26.8% for CHIP, representing $4.3 billion.[5]
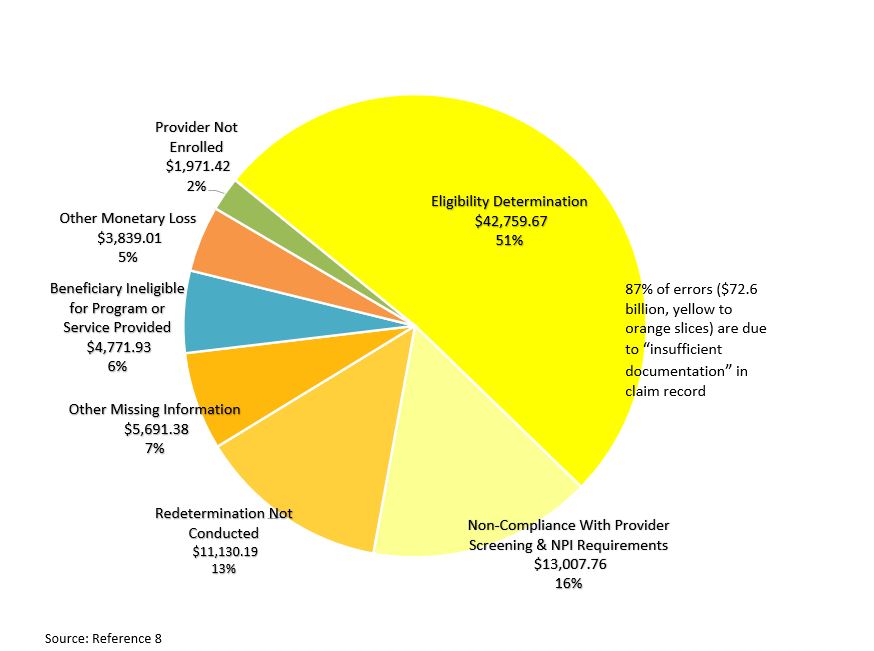
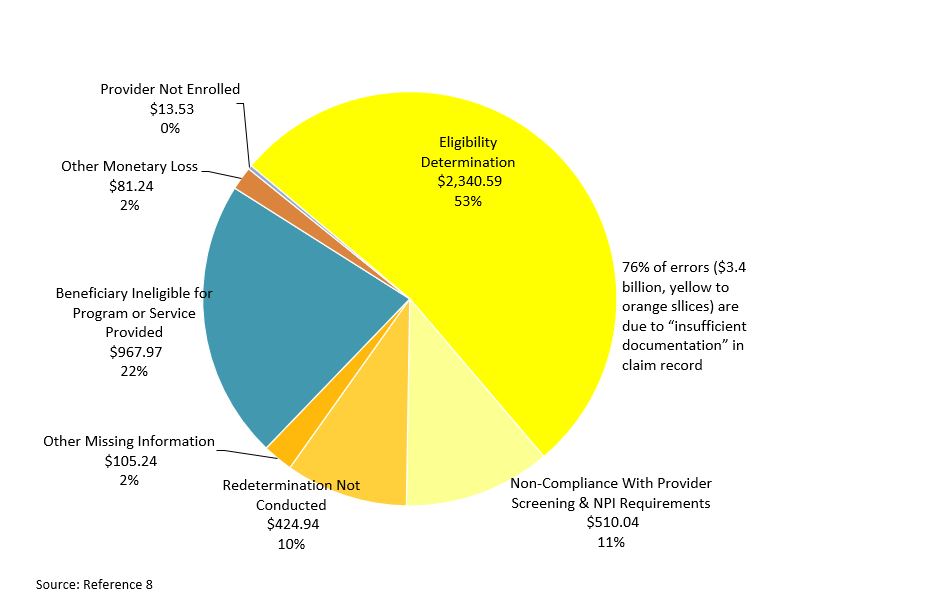
Most of the improper payments identified—about 87%, or $72.5 billion for Medicaid and 76%, or $3.38 billion, for CHIP—were due to “insufficient documentation” in the records examined.[6]
In the case of missing information, if that information had been on the claim and/or the state had complied with eligibility requirements, then claims might have been valid and payable. Conversely, any missing documentation might have affirmatively indicated that a provider or beneficiary was ineligible for Medicaid reimbursement and, therefore, the payment had been made in error. But it is very unlikely that all missing information would have been adverse.
Still, there is much to be gleaned from a deep dive into reasons behind “insufficient documentation,” as the following insights offer.
Pearls from PERM #1: Insufficient eligibility documentation
For both Medicaid and CHIP, eligibility issues with missing documentation dominate the improper payment assessments. Figures 1 and 2 illustrate four categories that can be grouped as “insufficient documentation” (the orange and yellow shades) account for most of the improper payment rates.
Notably, “eligibility determination was missing from the state’s system” accounted for more than half of the insufficient documentation errors for both Medicaid and CHIP.
As stakeholders that are engaged in unwinding initiatives pursue multifaceted campaigns with redeterminations, a deep dive into the supplemental data can support redetermination initiatives. For example:
-
“Signature not on file” was the second highest reason in terms of the number of errors and federal improper payment rate ($3.5 billion for Medicaid) and the highest reason for CHIP in terms of federal improper payment rate ($877.4 million) for beneficiary eligibility determination errors. Addressing this one issue alone could be impactful.[7]
-
Eligibility reviews were predominantly attributable to caseworker mistakes during enrollment or redeterminations. Caseworker errors were estimated to account for $32.5 billion in Medicaid and $2.1 billion in CHIP improper payments.[8] Training/retraining, enhanced desk aids, reduced caseloads, or other caseworker-related corrective actions might prevent such errors in the future.
-
Other noncompliance with eligibility requirement errors include determining a beneficiary to be eligible for the incorrect entitlement category (resulting in an eligible service or incorrect federal reimbursement being paid); not conducting redeterminations (timely or at all); or not performing, completing, or providing sufficient documentation to support a required element of the eligibility determination process.[9] These issues seemingly lend themselves to consideration of additional validation measures, potentially also from eligibility contractors and/or IT contractors. The compliance of states and their stakeholders will be essential to protecting eligible beneficiaries from erroneous terminations.
-
Both programs’ lack of compliance with provider eligibility accounted for roughly 18% of Medicaid PERM rates in Figure 1 and more than 10% of the CHIP PERM rates in Figure 2. When managed care organizations are used to administer Medicaid and/or CHIP, provider eligibility validation measures might need to be strengthened in contracting or auditing.
Pearls from PERM #2: Insufficient provider documentation
Compliance starts with documentation, and the predominance of the lack of such indicates room for improvement in several areas to consider:
-
Nearly $800 million in federal PERM across Medicaid and CHIP programs were due to providers not responding to requests for records.[10] Hospitals and health systems can support compliance with these requests to help reduce error rates.
-
Primary reasons for Absent Documentation included daily progress notes, attendance logs, flowsheets, worksheets, and records for Medicaid and CHIP, treatment plans, and goals.
-
Missing Documentation is the primary cause of improper payment determinations among medical record reviews (for FFS claims under such review).
Electronic record submittal systems that are routine today and electronic health records systems support reliability science, making it easy to do the right thing every time through forced process flows. But hospitals and health systems should consider additional validation measures, especially in the absence of those systems or the inability to capture all that is required for compliance to minimize these straightforward errors.
Pearls from PERM #3: Targeted providers
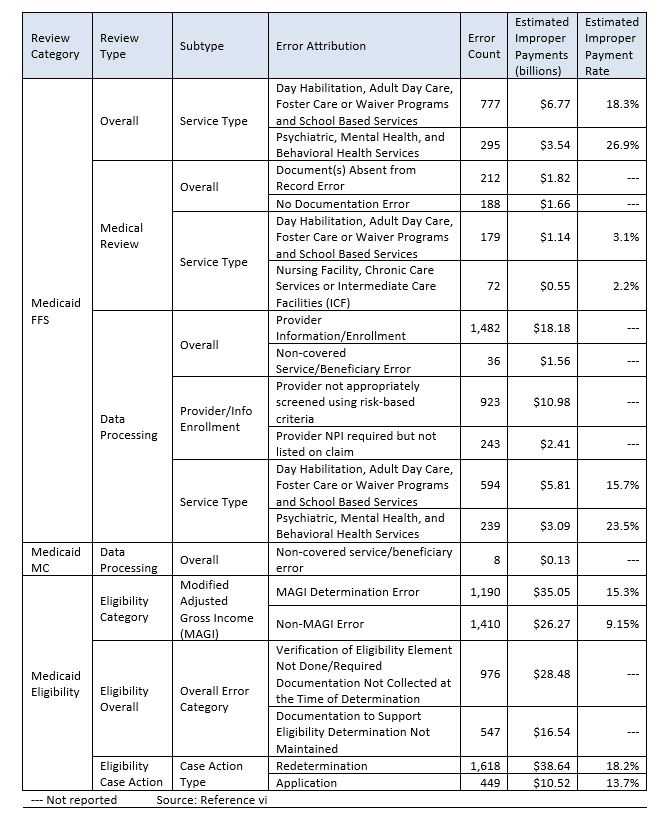
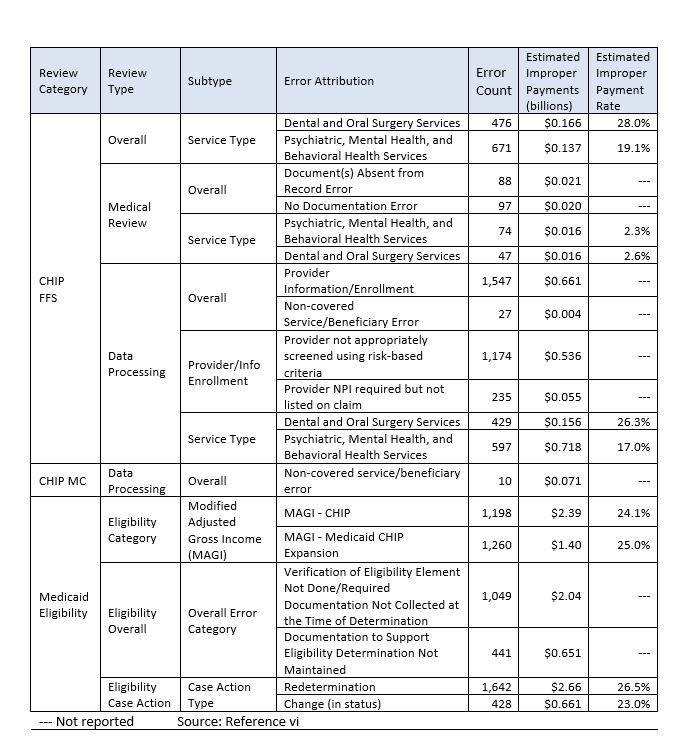
Among the provider types that had the highest number or percentage of documentation errors were:
-
Behavioral Health service providers (both Medicaid and CHIP programs)
-
Day Habilitation/Adult Day Care/Foster/Waiver/School-based providers (Medicaid)
-
Dental providers (CHIP)
Tables 1 and 2 detail the most frequently reported and highest cost errors in Medicaid and CHIP, respectively.
Additional training sessions, monitoring, and other corrective action to improve compliance will be needed for these providers as the nation continues to aggressively move to waivers and home- and community-based services reflecting the aging population and the nation’s recognition for noninstitutionalized settings. Also, as the nation implements Administration mental health initiatives released at the end of 2022, including school-based care, these providers will take on increasing importance, and thus, their compliance could have a greater impact on future PERM rates.
The same holds true for dental providers as states add dental benefits to Medicaid per the American Dental Association’s push in the last two years. Like many things, practice makes perfect or at least closer to perfect: The CHIP federal improper payment estimate is half the error rate of Medicaid; CHIP has required dental providers to participate in the program longer than Medicaid dental providers.
Looking forward
It is anticipated that the PERM program error rates for Medicaid and CHIP will only increase in the next reporting cycle, at least as unwinding exacerbates eligibility redetermination administrative errors. Indeed, while 2022 PERM rates were lower than the previously published year due to COVID-19 review flexibilities and corrective actions, the rates are still higher than the Payment Integrity Information Act (PIIA) of 2019’s <10% threshold. And CMS anticipates rates will remain above the 10% threshold until at least 2025.[11] Indeed, within HHS, only Medicaid and CHIP exceed the PIIA’s improper payment threshold.
Under PIIA’s microscope, CMS is induced to reduce rates as quickly as possible while facing increasing scrutiny. (Each consecutive year that an agency’s programs exceed thresholds results in increasing penalties.) And reducing largely administrative error rates will require all those involved in Medicaid program integrity, which starts with compliance, to support corrective action.
States already have help in the Medicaid Integrity Institute, cross-enterprise sharing, and other technical assistance CMS offers to support correction action plans. A deep dive into each state’s own PERM data may reveal error patterns that could benefit from further root cause analysis and solutions. Also, knowledgeable additional resources can help stakeholders enhance or develop new corrective actions and can offer direction to improve during one of the most significant times in Medicaid’s programmatic history.
Takeaways
-
National and newer state-level Payment Error Rate Measurement (PERM) data deep dives can support unwinding and other current initiatives.
-
Compliance starts with documentation, yet insufficient documentation is a critical contributor to PERM rates. Hospitals and health systems can support improved documentation.
-
Missing signatures on file were a key reason for eligibility error rates.
-
Behavioral health, dental, and other certain providers should receive focused attention as they are increasingly used yet perform poorly in compliant documentation.
-
The Centers for Medicare & Medicaid Services will be keen on reducing error rates as quickly as possible due to the consequences of missing thresholds of the 2019 Payment Integrity Information Act.

